
Stillbirth is a pathology of pregnancy when the fetus dies in utero in the 20th week of pregnancy or after it (we should remind you that a loss of a baby before the 20th week is considered a miscarriage). About one of 260 pregnancies ends with stillbirth. The majority of stillbirths happen long before the due date, but there are some cases when the baby dies during childbirth.
Diagnostics of Stillbirth
An expectant mother may notice that her baby has stopped moving and consult her doctor about it as well as she may find out about stillbirth during the ordinary pre-natal visit.
The gynecologist listens to the heart of the fetus during the usual examination with the help of portable Doppler ultrasound. If there is no heartbeat the doctor prescribes the woman an off-schedule ultrasound of the uterus and fetus to confirm that the fetus’s heart has stopped and the baby is dead.
Sometimes the ultrasound provides information that helps to understand why the baby has died. The gynecologist also usually makes an appointment for a woman to pass a blood test to determine possible causes of stillbirth.
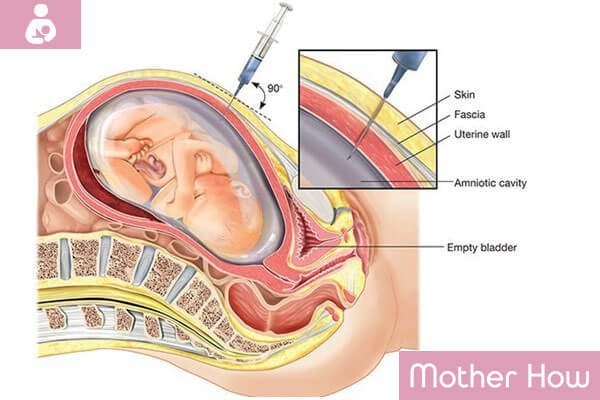
Besides, you may be sent to amniocentesis (amniotic fluid test) to check if the baby had any chromosome problems which might have led to stillbirth. Why should you do amniocentesis if the baby is already dead? The point is that the amniotic fluid test gives the fullest information about your child’s chromosomes; it’s even better than the analysis of tissue samples after stillbirth.
Extraction of the Stillborn Child
According to the medical evidence, women with this diagnosis are having an immediate abortion or given time to prepare. At that time, the woman is observed by a gynecologist to rule out the risk of infection or blood-dotting disorder. The majority of women prefer to extract the stillborn fetus by the delivery or abortion immediately after they find out about the death of their baby. The women who have a choice between these two ways of extraction of the stillborn fetus should consider some important facts.
- Delivery: If the uterine cervix doesn’t dilate the doctor can encourage this process. The woman is injected with oxytocin to stimulate uterine contractions. Most women are able to give birth to a dead baby on their own. The delivery is chosen by those women who want to endure the birth as a way to bid farewell to the baby. In addition, the autopsy after the birth can give much more answers than after the abortion.
- Abortion: An experienced doctor helps to dilate the cervix of the uterus and extracts the baby while the mother is sedated. This is the best way for a woman who prefers a faster and more detached procedure. Under the condition of the doctor’s experience, in this case, the woman has fewer chances of complications than during delivery, though in both cases the risks are minimal.
The Causes of Stillbirth
- Slowed Development of the Embryo: If the embryo is developing slowly it can increase the risk of stillbirth.
- A Detachment of the Placenta: In this case, the uterine nutrients don’t come from the uterus to the baby and this leads to the death of the fetus.
- Congenital Defects: Chromosome and genetic anomalies, different structure malformations may also lead to stillbirth. Sometimes stillborn babies have several congenital defects.
- Infections: Infections of the mother, baby or placenta are another widespread reasons of stillbirth, especially if they happen before the 28th week of pregnancy.
- Umbilical Cord Anomalies: They occur more seldom, for example, a knot of the umbilical cord or the cord fastened badly to the placenta. It’s usually not dangerous, but sometimes causes the fetus’s hypoxia.
- Other Causes: such as the lack of oxygen during difficult childbirth or as a result of trauma (for example, car crash) may be the cause of a stillborn baby.
Precautions Against Stillbirth Before Conception
If you’re still not pregnant you should begin planning the conception with a visit to a doctor. This will give you the possibility to find out and cure any problems because they will be revealed during the examination. And if you’re suffering from such chronic diseases as saccharine diabetes or high blood pressure (arterial tension) you will be sure that these diseases will be controlled during pregnancy due to the visit to a doctor.
Your doctor should know about any medications you take so that if the need arises one medication will be replaced with another or the dosage will be corrected. And if you’re taking any bioactive dietary supplements or herbal teas and medications please don’t forget to ask your doctor if they are safe for future mothers.
Begin to take 400 mcg of folic acid per day (as a separate medication or as a component of poly-vitamins for the pregnant), and it’s better to take it at least a month before the supposed conception. The use of folic acid may considerably reduce the risk of the development of inborn defects of the neural tubes, particularly split spine.
If you suffer from adiposity, try to lose weight before attempting to become pregnant. But don’t ever try to lose weight by keeping a diet during pregnancy! Your gynecologist can help you to select a proper diet or send you to consult with an experienced dietitian.
Precautions Against Stillbirth During Pregnancy

First of all, don’t smoke, drink alcohol or take drugs during pregnancy. If you have problems with refusing cigarettes, alcohol, or drugs, ask your doctor for direction to an expert in narcology, who will help you quit these bad habits, and search for information on how to stop smoking during pregnancy. The research has shown that the women who stopped smoking before the 9th week of pregnancy have the same odds of stillbirth as non-smoking women.
Secondly, consult your doctor with any suspicious symptoms! For example, bleeding from the vagina may be a sign of the detachment of the placenta, miscarriage, and a whole lot of other disorders, dangerous for your pregnancy and your own health.
Besides the bleedings there are a few other symptoms with which you should immediately ask for medical aid – these are pains in the uterus, pains in the back, painful false contractions, or uterine contractions which don’t cease but become even more frequent and sudden decrease in fetus’s movements.
Your doctor may recommend you to count the number of the baby’s stirs every day since the 28th week of pregnancy. If you count less than 10 stirs during two hours or if you feel that your baby is moving less than usual, immediately consult a doctor!
If you had cases of stillbirth before (or if there is a high risk of it due to any other reason) your condition and the condition of your baby will be thoroughly observed during the whole period of pregnancy and since the 32nd week of pregnancy, the following tests will be conducted: heartbeat monitoring, cardiotocography, and ultrasound. If the results will show that your baby will be better outside the uterus than inside of it, you will be stimulated for childbirth or endure a Caesarean section.
What if Stillbirth will Happen Again?
You have already had experienced the tragedy of stillbirth and are afraid of another case of it now? If your doctor found out the cause of prenatal death of the baby and it was eliminated the odds of stillbirth happening again are extremely low.
But such a possibility is much higher if you have such chronic diseases as, for instance, lupus, hypertension, or diabetes, or if you’ve got any complications of pregnancy that are making the threat of stillbirth, even more, real (for example, the detachment of the placenta).
Before trying to become pregnant after stillbirth discusses all possible risks with your gynecologist and prepare as thoroughly as possible for the conception!
How to Cope with Stillbirth?
Accepting stillbirth is a hard challenge for unfortunate parents because in the case of such short, in fact barely begun life it’s even more difficult to find any sense in death than in any other case. The thought of severe malformations that wouldn’t give the child any chance of normal life may, in fact, have a consolatory effect on parents.
Speaking of particular measures, in this case, the most important thing is to properly bid farewell to the baby. Instead of stuffing the mother with sedatives and sending the father home, the doctors should give the parents the possibility to look at the baby one last time and say their goodbyes, to carry out a proper funeral. The bed for the father should be placed in the mother’s ward because now they really need each other.
A sense of relief from the parents’ grief and despair can be brought by the acceptance of their own mortality. They should realize and accept that death is closely bound to life and is a natural opposite to it. The one that admits the death to be a matter of time for every being easier finds consolation.
Group therapy that helps to deal with stillbirth is sometimes necessary for a woman faced with such misfortune. The women who experienced these problems in the past can be of better help to others than professional therapists sometimes. If such groups can’t bring any relief, then maybe psychotherapy should be considered.

Born in Belarus, 1985, a pedagogue and family psychologist, mother. Taking part in procedures of social adaptation of the foster children in new families. Since 2015 is a chief editor of the motherhow.com project, selecting the best and up-to-date material for those, who are planning, expecting, and already having babies.